For nearly a decade, healthcare staffing has been having an argument with itself.
Everyone agrees technology will make the industry more efficient. The disagreement is how much of staffing is really a relationship business, and how much can be reduced to quantifiable outcomes. Can software ever do what a great recruiter does at 4:30 AM, when an ICU shift opens and a charge nurse is one name away from a safe night?
In my opinion, it was never really a debate.
Every services-heavy industry has had the same argument, and they’ve all resolved it the same way. Taxis. Freight. Lodging. Financial services. The relationship layer doesn’t disappear. It moves out of the broker and into the infrastructure that makes the transaction trustworthy at scale. The 4:30 AM call still happens. By the time someone picks up the phone, the system already knows who’s qualified, credentialed, available, and likely to pick up. Most of the time, the phone never has to ring.
What’s new in this generation is what becomes possible after the argument resolves. Once the workflow is software, frontier AI doesn’t just automate the existing motions a little faster. It runs them.
A workforce in crisis: the biggest line on every hospital’s budget
The healthcare workforce is under structural strain on both ends of the supply curve.
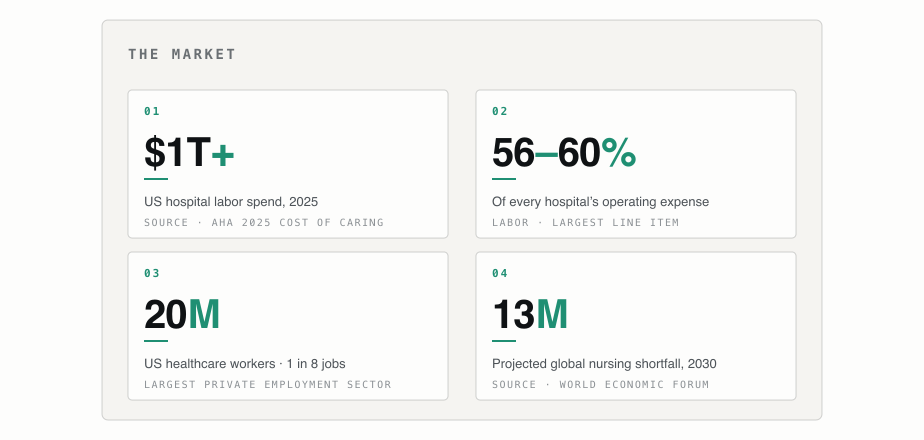
Demand is rising sharply under an aging population and a broadening definition of what counts as healthcare. Supply is contracting under retirements, burnout, and a thin new-entrant pipeline. The global nursing shortfall alone is projected at more than 13 million by 2030.
The numbers are worth pausing on. Healthcare is now the largest private employment sector in the United States. Roughly 20 million people work in it; about 1 in 8 American jobs. Hospital labor spend crossed $1 trillion in 2025. Labor is 56 to 60% of every hospital’s operating expense, the largest line item on the income statement of an industry approaching one-fifth of US GDP. No other operational decision a hospital makes carries comparable weight. Nothing comes close.
For most healthcare employers, the majority of clinical staff are permanent employees on fixed schedules. Sick leave, FMLA, census surges. Every day produces open shifts the schedule didn’t anticipate. Hospitals try to plug the gap with contingent labor: per diem locals picking up extra shifts, travel clinicians on three-month contracts. Both are expensive, slow to source, and most effective with lead time hospitals rarely have.
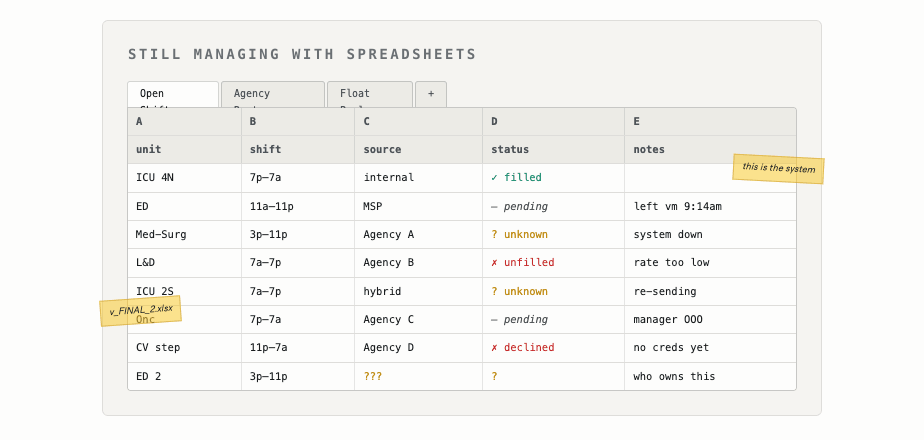
What remains falls to a nurse manager with a phone and a handful of levers: shift bonuses, text message requests sent in hope, last-minute calls and emails. The result is predictable. Labor cost climbs. Stress climbs with it. Morale and retention erode, accelerating the same supply problem the system was trying to manage. The biggest budget line in healthcare is being managed with the lowest-tech infrastructure in the building, by people whose actual job is to take care of patients.
No HR, nursing, or finance leader, given a clean sheet of paper, would design the system hospitals run today.
Today’s solutions all predate the World Wide Web. None was designed for an industry that flexes labor across W‑2, contract, per diem, and gig employment in real time. None was designed for AI. And yet this is the stack that fills the shifts in every operating room, ICU, ED, and inpatient unit in the country.
Internal labor is managed by one set of tools. External labor is managed by another. Each external pathway (per diem, travel, locums, allied) routes through different agencies, often with a Managed Service Provider (MSP) sitting on top to manage them. Hybrid programs get built from scratch. Most of the actual coordination happens in spreadsheets, in email, and on the phone.
What hospitals actually care about
Strip the noise out of how this is talked about, and healthcare employers care about three measurable things:
Fill rate: the percentage of open shifts that are adequately staffed.
Labor cost: direct compensation plus the indirect cost of incentives, agency markups, overtime, and intermediation.
Quality of care: the outcome everything else exists to produce.
These aren’t separate problems. They’re three views on the same one. A good labor system improves all three simultaneously. Any system that trades one off against another isn’t solving the underlying problem; it’s relocating the bill.
The system that has to exist hasn’t existed.
The operating system for the healthcare workforce
That’s what we’ve spent nearly a decade building.
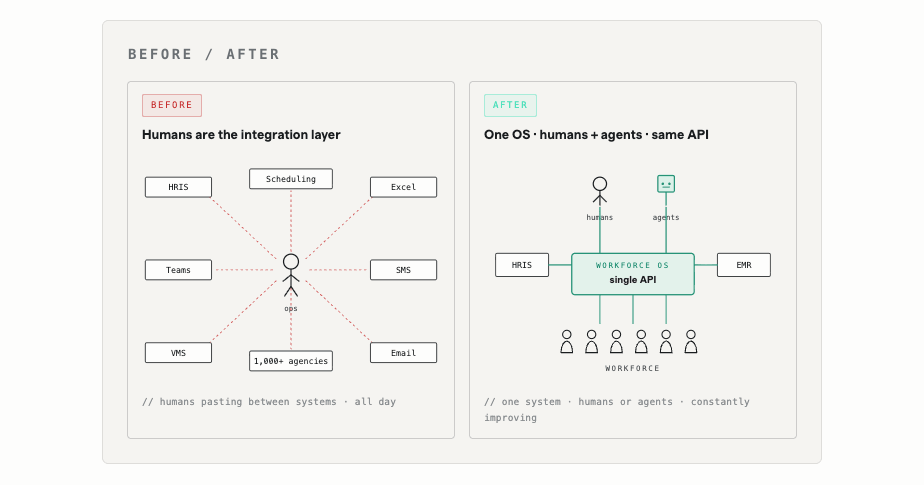
It replaces multiple categories of incumbent tools at once. Not a better staffing agency. Not a better VMS (Vendor Management System). Not a better scheduling system. The orchestration layer that sits above all of them, and increasingly, the layer that makes most of them unnecessary.
We call it the operating system for the healthcare workforce because structurally that’s what it is. An OS is the shared substrate every other piece of software runs on. It knows the state of every resource being coordinated, mediates every transaction, and exposes clean interfaces to applications that want to do useful work on top of it.
Apply that to clinical labor and the analogy stops being an analogy. One system that knows every shift, every clinician, every credential, every match, every contract. One system that mediates the transactions between hospitals, clinicians, agencies, and internal float pools. One system that exposes the interfaces (for nurse managers, clinicians, partner agencies, and increasingly AI agents) that turn raw coordination into filled shifts.
An OS at this scale, in this industry, can’t be pure software. Sequoia’s Julien Bek recently argued that the next generation of trillion-dollar companies won’t sell software at all. They’ll sell the work.
For every dollar spent on software, six are spent on services. --- Bek Abdullayev
The opportunity isn’t a better tool for the people doing the work. It’s the outcome the tool was a proxy for: what Bek calls the autopilot instead of the copilot.
Healthcare workforce services---the staffing agencies, MSPs, credentialing back offices, scheduling consultancies---are a layer worth tens of billions of dollars. It exists because the underlying software has never been good enough to deliver the outcome on its own. The opportunity isn’t a better workforce tool. It’s the filled shift. That’s the operating system that the healthcare industry needs.
Network. Intelligence. Rails.
The right operating system has three irreducible components, mapping to the three jobs every healthcare employer needs done: access to enough supply, matching supply to demand, and running the logistical workflows that turns a match into a filled, paid, credentialed, compliant shift. Take any one out and the system collapses into something that already exists.
| Network | Intelligence | Rails | |
|---|---|---|---|
| Job to be done | Access to enough supply | Match supply to demand, continuously | Turn a match into a filled, paid, credentialed shift |
| What it covers | Internal staff plus every external pathway on one substrate | Forecasting, dynamic pricing, clinical and preference matching | Credentialing, contracts, scheduling, invoicing, payments |
| What collapses without it | Decisions with no labor to execute against | A directory with no autopilot | A recommendation engine with no way to execute |
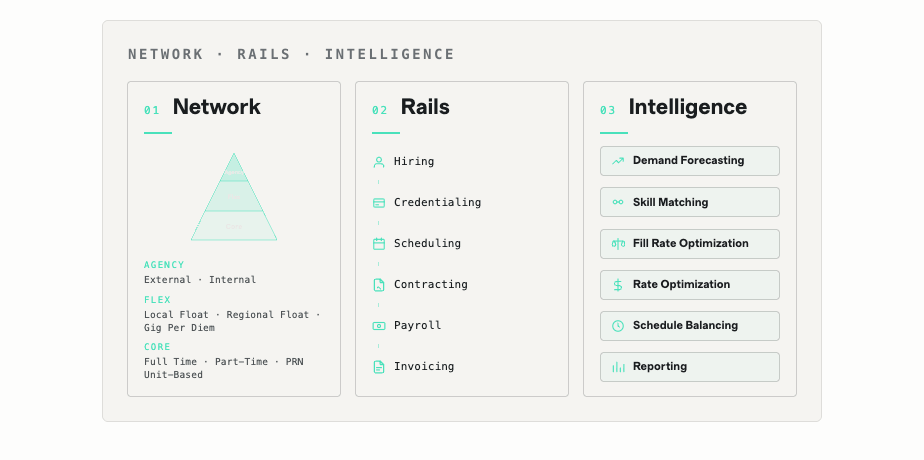
Network: access to enough supply. A hospital’s complete labor pool, internal staff and every external pathway (per diem, travel, agency, gig), unified on one substrate. Without a network that spans both sides, the system has decisions but no labor to execute against. The external side has to be deep enough to cover every employment model in real time. The internal side has to live in the same system as the external, so a shift can route to either pool without translation. And the network has to keep growing: at scale, recruiting, qualifying, retaining, and re-engaging clinicians is itself an autopilot problem. The same intelligence that fills shifts grows and rebalances the network underneath.
Intelligence: matching supply to demand, continuously. The agentic layer that forecasts labor need, prices open shifts in real time, and matches clinicians on both clinical fit and individual preferences. This is where the autopilot is most visible. Forecasting demand for a unit months out. Pricing shift incentives dynamically against the local labor market. Routing the right clinician to the right shift at the right time, while avoiding the schedules that push clinicians toward burnout. Proactively hiring contract workers to fill foreseeable gaps. The objective isn’t just filling shifts. It’s filling them in ways that respect clinician preferences and reduce burnout, the things that actually keep clinicians in the workforce.
Rails: the logistical workflows that turn matches into filled shifts. Validating and monitoring credentials. Executing contracts within policy. Approvals, scheduling, applicant tracking, invoicing, payments, supplier management. Automated where possible, AI-assisted where judgment is required. Without rails, you have a recommendation engine with no way to execute. The hard architectural ask is coordinating internal and external labor on one plane, in one data model, with one view of cost and utilization across every fulfillment channel.
A staffing company has the network and almost nothing else. A VMS has rails for one labor type. A scheduling system has rails for internal labor. HR platforms have some rails but no clinical depth and no clinician network. None of them has all three components. The compounding value comes from the data the three produce together: the substrate AI needs to actually deliver the outcome.
What this lets hospitals and clinicians do
With the OS and AI together, the math on hospital labor changes. Hospitals can finally operate their largest cost center with the precision they apply to every other major operational decision. Fill rates rise. Labor costs come down. Quality of care, which is what all of this is finally for, becomes more consistent. The labor pipeline that produces it is more reliable.
Once the OS exists, the multi-layer intermediation that defined the old model compresses. Multiple vendors. The spreadsheets stitching things together. The team of people whose job is (or shouldn’t be) playing Tetris with staff. Those middle layers exist because no system could coordinate the whole surface. There is now. Removing them makes the system faster for hospitals and cheaper to operate.
More importantly, it makes the experience meaningfully better for clinicians: higher pay, because the margin previously captured by intermediation flows through; faster matching, because the system is doing the work continuously instead of waiting on a phone tree; and a far simpler way to find and accept the work they want.
Where this goes
Within ten years, every clinical workforce will be powered by an operating system. Software made it possible. AI is accelerating it. It is not a copilot. It is not a recommendation engine. It’s the system that does the work.
Healthcare staffing as it has been measured for thirty years will look different in five. The framing of agencies versus internal staff will collapse, because the OS doesn’t care which side of that line a clinician sits on. The economics that made the existing healthcare staffing leaders so prominent (margin spread on travel contracts) will compress, because the layer above them commoditizes the work. As a result, companies rebuilt around this layer will look very different from the ones that defined the previous era.
Trusted’s mission is to help people everywhere get care. Getting the right clinicians to the right patients at the right moment is the gating constraint on that mission, for our customers, for our industry, and for the patients on the other end of every shift.
Check out our OS for the healthcare workforce at works.ai, and our flexible jobs marketplace for clinicians at trustedhealth.com.
--- Lennie, Founder